
Case 82
- Wangpan Shi
- Mar 18
- 1 min read

A 78-year-old male with a cervical lesion.



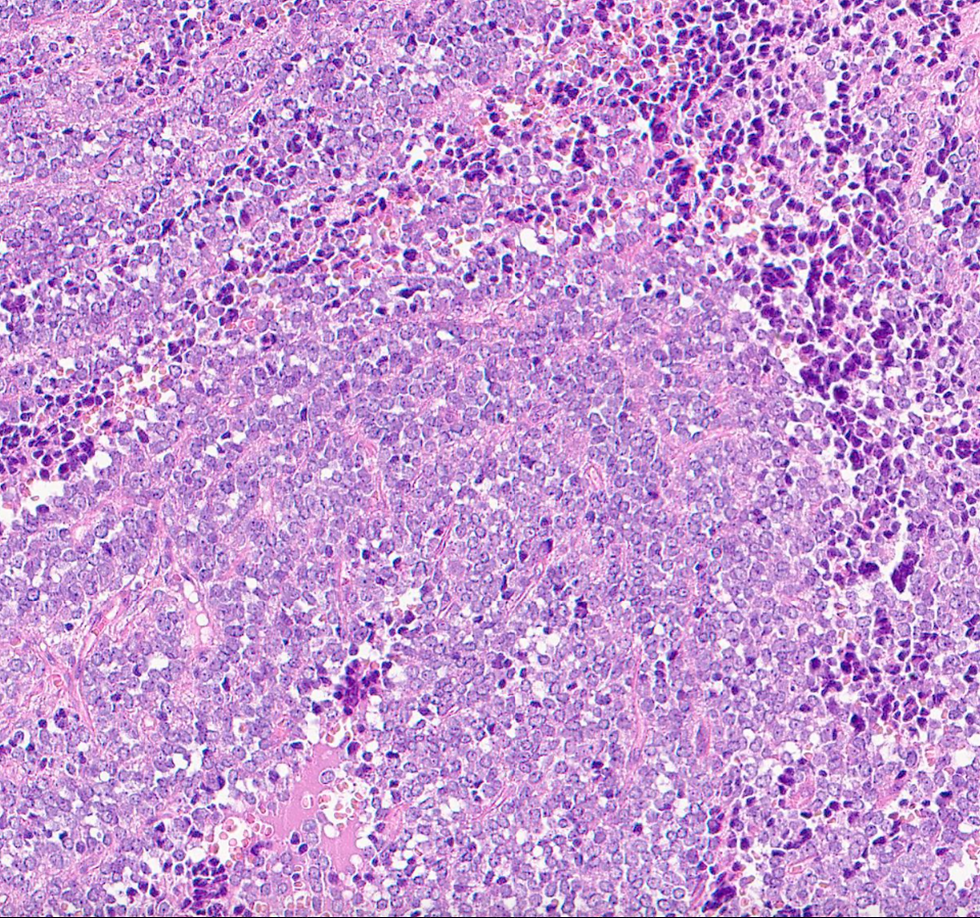


If the tumor is positive for CD99, what's the diagnosis?
A: Ewing sarcoma
B: Neuroendocrine carcinoma
C: Merkel cell carcinoma
D: HPV-related poorly differentiated carcinoma
Answer
This is a case of Ewing sarcoma. NKX 2.2 is the best sensitive and specific marker for Ewing sarcoma.
Key Features Supporting Ewing Sarcoma Diagnosis:
Histologic Features:
Monotonous small round blue cells arranged in sheets or solid aggregates.
Fibrous septa separating tumor cells.
Focal rosettes may be present.
Round nuclei, coarse chromatin, small nucleoli.
Cytoplasm ranges from scant to abundant and may be eosinophilic or clear.
Brisk mitotic activity.
Common necrosis.
Immunohistochemical Profile:
Strong, diffuse membranous CD99 expression (hallmark feature of Ewing sarcoma).
Nuclear FLI1 expression (consistent with Ewing sarcoma family tumors).
Focal positivity for broad-spectrum cytokeratins (seen in some cases).
Negative for desmin, myogenin, and MYOD1 (excludes rhabdomyosarcoma).
Molecular Features:
EWSR1::FLI1 fusion (t(11;22)(q24;q12)) is the most common translocation.
Other less common translocations include EWSR1::ERG (t(21;22)(q22;q12)).
Differential Diagnosis:
Lymphoblastic lymphoma → Negative for CD99, positive for TdT.
Rhabdomyosarcoma → Positive for desmin, myogenin, MYOD1.
Neuroblastoma → Positive for synaptophysin, negative for CD99.
Synovial sarcoma (monophasic type) → May be positive for CD99 but shows SYT-SSX translocation.
Case credit: https://qp.91360.com/9817.html?lang=en
Author: Wangpan Jackson Shi, MD
Comments