
Case 12
- Wangpan Shi
- Jan 10
- 2 min read

Updated: Jan 23
A 70 year old male was found to have a exophtic bladder lesion. TURBT specimen of the lesion is shown below:
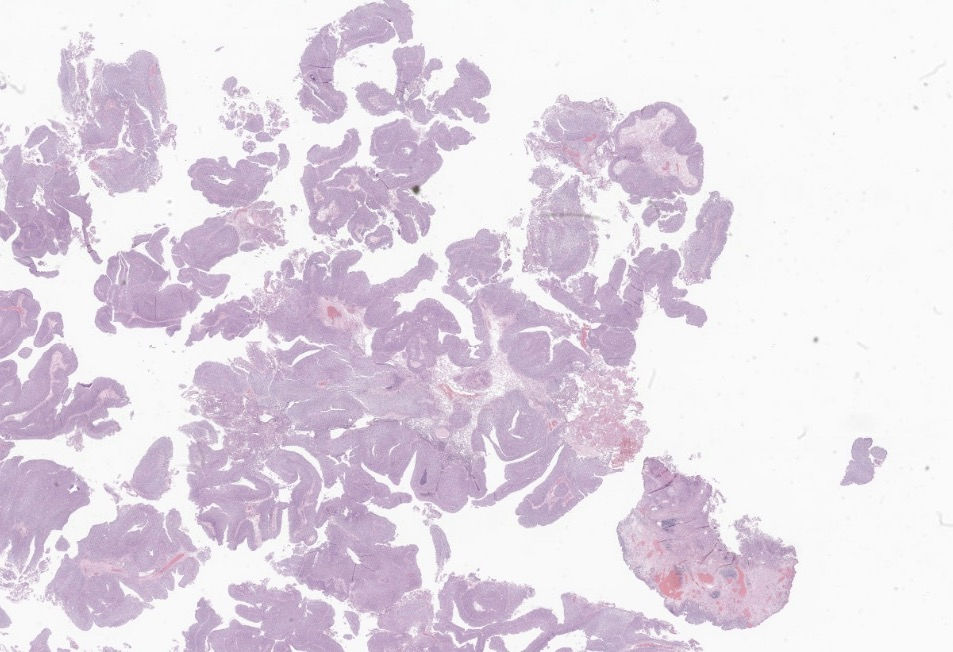




What's the diagnosis?
A: Non-invasive papillary urothelial carcinoma, low-grade
B: Non-invasive papillary urothelial carcinoma, high-grade
C: Urothelial papilloma with focal reactive atypia
D: Papillary urothelial neoplasm of low malignant potential
E: Urothelial carcinoma in situ
Answer
The correct answer is non-invasive papillary urothelial carcinoma, low-grade. This could be a highly subjective area. A summary of key features for the differential diagnosis by WHO is shown below:
1.Urothelial papilloma: slender fibrovascular cores covered by urothelium of normal thickness (<7 cells) with normal cytological features.
2.Papillary urothelial neoplasm of low malignant potential: no history of urothelial carcinoma; fibrovascular papillary structures lined by urothelium that is thickened or shows increased cellularity; mild cytological atypia. People rarely diagnosed PUNLMP.
3.LG: fibrovascular papillary cores or expanded and inverted nests, lined by urothelial cells with (at most) mild cytological atypia and architectural disorder; absence of marked nuclear size variation and hyperchromasia
There is very mild to none loss of polarity in LG
4.HG: papillary structures or sheets of urothelium with marked cytoarchitectural disorder- papillae with fusion and frequent branching. Nonetheless, the cytological features – not the architectural pattern – determine the high-grade nature of the lesion. Disorderly orientation with loss of polarity. They display irregular and pleomorphic nuclei that are readily apparent at low to intermediate magnification. Significant nuclear size variation, nuclear hyperchromasia, prominent irregular nucleoli, and irregular nuclear contours are evident features. Frequent mitoses including irregular forms are usually noted. Nuclear anaplasia can be occasionally encountered
Back to this case, the tumor is definitely thickened, showed maintained polarity, no marked nuclear size variation, and of note mitosis is not part of the grading system although a marked elevation in mitosis should be interpreted cautiously. In this case it's elevated but mostly near basal layer.
References: https://tumourclassification.iarc.who.int/chapters/36/68. Some of the words are directly from WHO for only education purposes.
Case credit: UCSD Pathology
Author: Wangpan Jackson Shi, MD
Comments