
Case 2
- Wangpan Shi
- Jan 5
- 2 min read

Updated: Jan 23
A 30-year-old female with an incidental finding of supraclavicular mass with calcification.


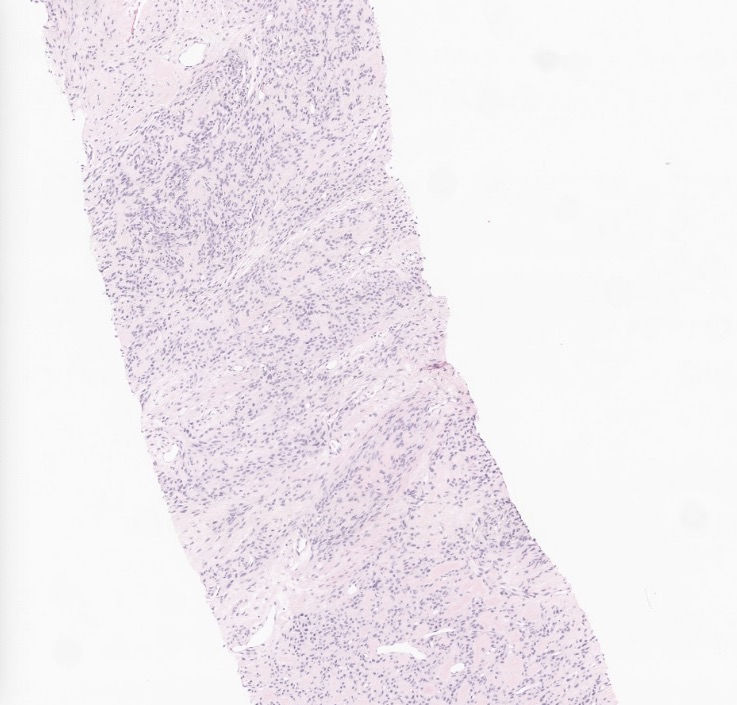



What's your morphological impression at this point?
A: Nodular fasciitis
B: Atypical fibroxanthoma
C: Low grade fibromyxoid neoplasm
D: Low grade fibromyxoid sarcoma
E: Myxoma
F: Solitary fibrous tumor
G: Ossifying fibromyxoid tumor
H: Angiofibroma of soft tissue
I: Myxoid diffuse neurofibroma
Answer
Tumor with fibromyxoid morphology can all be the differentials. diffuse CD10 is a clue but this case does not represent a classic morphology in textbook. Stay tuned for IHC and molecular!
An extended IHC panel showed the tumors are positive for CD10 only,
while negative for CD34, STAT6, SOX10, S100, MUC4, SMA, myogenin,
beta catenin (nuclear staining), p63, and pankeratin. RB1 is retained. The
tumor cells are focal and weakly positive for ER and desmin.
What's the diagnosis?
A: Nodular fasciitis
B: Atypical fibroxanthoma
C: Low grade fibromyxoid neoplasm
D: Low grade fibromyxoid sarcoma
E: Myxoma
F: Solitary fibrous tumor
G: Ossifying fibromyxoid tumor
H: Angiofibroma of soft tissue
I: Myxoid diffuse neurofibroma
Answer
By this immunoprofile, SFT, LGFMS, angiofibroma, diffuse neurofibroma can be confidently excluded. However, it still does not help much. Stay tuned for molecular findings.
Case was sent to sarcoma fusion panel and NBPF10::PHF1 fusion was detected. What are the tumors associated with this fusion?
A: Ossifying fibromyxoid tumor
B: Superficial acral fibromyxoma
C: Chondromyxoid fibroma
D: Intramuscular myxoma
E: Cutaneous nerve sheath myxoma
F: Myxofibrosarcoma
Answer
The final correct answer is A. Ossifying fibromyxoid tumor. It's a benign mesenchymal neoplasm of uncertain differentiation that at least 50% of it harbors PHF1 fusion. The hallmark by morphology is uniform, oval to round tumor cells in myxoid, fibromyxoid or hyalinized stroma with lobulated or nodular growth pattern and frequent incomplete / partial rim of metaplastic bone. In this case, we don't see any of the metaplasitc bone rim. By IHC, the tumor can be positive for CD10 and S100, while negative for CD34, STAT6, SOX10, and MUC4. The common molecular fusion variants are EP400-PHF1, MEAF6-PHF1, EPC1-PHF1, and PHF1-TFE3. A few fusions involving BCOR, BCORL1, CREBBP, and/or KDM2A have been described, especially in malignant OFMT. Superficial acral fibromyxoma has RB1 loss; Chondromyxoid fibroma has GRM1 upregulation. There is a high prevalence of GNAS (exons 8 and 9) point mutation in sporadic intramuscular and cellular myxomas. No genetic abnormality has been described to date for term nerve sheath myxoma. Myxofibrosarcoma showed complex karyotypes, with intratumoural heterogeneity and chromosome numbers in the triploid or tetraploid range in most cases.
References:
https://www.pathologyoutlines.com/topic/softtissueossifyingfibromyxoid.html
https://tumourclassification.iarc.who.int/chaptercontent/33/117
Folpe AL, Weiss SW. Ossifying fibromyxoid tumor of soft parts: a clinicopathologic study of 70 cases with emphasis on atypical and malignant variants. Am J Surg Pathol. 2003 Apr;27(4):421-31. doi: 10.1097/00000478-200304000-00001. PMID: 12657926.
Miettinen M, Finnell V, Fetsch JF. Ossifying fibromyxoid tumor of soft parts--a clinicopathologic and immunohistochemical study of 104 cases with long-term follow-up and a critical review of the literature. Am J Surg Pathol. 2008 Jul;32(7):996-1005. doi: 10.1097/PAS.0b013e318160736a. PMID: 18469710.
Case credit: UCSD Pathology
Author: Wangpan Jackson Shi, MD
Comments